[Posted by Roy]
I attended yesterday's hearing, missing the FDA's presentation in the morning, but arriving for the public comments part and the afternoon deliberations. (Check out the FDA's 150-page .pdf testimony.) I was also among the 75 people who provided testimony to the committee. The meeting lasted a total of 9.5 hours!
This is the first time I've been to an FDA Advisory Committee meeting. These are public meetings (required to be public, by law) in which the committee members discuss the issues and make decisions. The FDA presents data to them; in this case, it was data from numerous clinical trials solicited from big pharma to especially get at the question of induction of suicidal thoughts or behaviors by antidepressant medications. After the committee hears these data, they listen to public testimony. After that, they discuss what they heard, and respond to the FDA's recommendations in the form of support, opposition, or other recommendations.
The committee is advisory in nature, meaning that the FDA takes what they say into consideration, but is not bound by their recommendations. The FDA does typically follow their recommendations. Three of the committee members could not vote due to conflicts of interest (receiving industry funds for clinical research and such).
In this post, I will first cut to the chase and tell you what the committee's recommendations were. In a second post, I'll give you more details to flesh out some of the discussion points and concerns that the committee raised, and also discuss the public testimony, some of it being very gut-wrenching and impassioned.
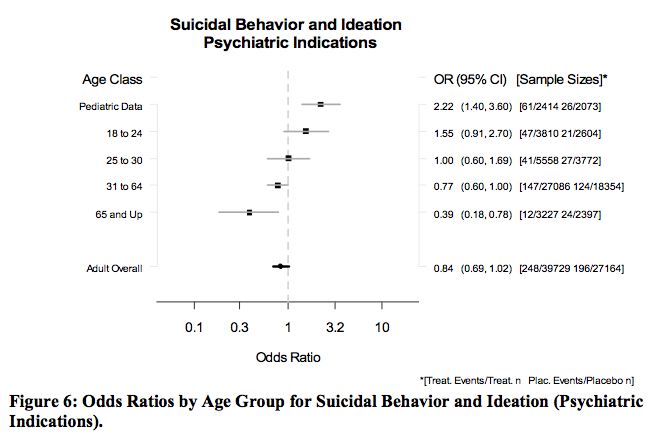
If I had to choose one image that best describes the entire hearing, it is the one above.
What this demonstrates is that as age goes up, the relative risk of suicidal thoughts or behavior goes down. The numbers plotted are the Odds Ratios... meaning that, compared to the folks taking placebo, what are the odds that those taking antidepressants are likely to have either thoughts of suicide or actual suicidal behavior. So, an O.R.=1 means that the chances are the same, which means no difference. An O.R.=2 means your chance is doubled. An O.R.=0.5 means your chance is halved. The black square is the estimated O.R., and the gray bar represents the 95% Confidence Interval... meaning that the statistical probability of the true O.R. being within the gray bar is 95%. Thus, if the gray bar touches 1 (the vertical dashed line), then the two groups (placebo and medication) are NOT statistically significant. If they do not touch 1, then they ARE statistically significant. Got it? To put it most simply, left of the dashed line is good, right of the line is bad.
So, the pediatric Odds Ratio does not include 1; this result supports the decision made in 2004 to add a black box warning that says these medications are associated with an increase in suicidal thoughts or behavior. (As it turns out, it is just thoughts, not behavior, but I'll address that in the second post.)
The 18-24 year-old Odds Ratio does include 1 (0.91-2.70), thus we cannot say that there is an increased risk.
The 31-64 year-old Odds Ratio just includes 1, but the estimated O.R. is less than 1, meaning that we cannot say there is a decreased risk, but there almost is.
For the over 65 group, there is clearly a significantly decreased risk of suicidal thoughts or behaviors. Note that these appear to be rare events... 12 people out of 3227 taking medication, and 24 out of 2397 taking placebo reported suicidal thoughts or behaviors. Hard to believe that only 1% of people with major depression had suicidal thoughts, huh?
Okay, so here is what the committee decided:
- There is a clear relationship between age and suicidal thoughts or behaviors in people taking antidepressants.
- Keep the black box warning that currently exists, but be very cautious about discouraging depression treatment and attempt to include balancing language that states that the risk of suicidal thoughts or behaviors when not taking medications should be considered. (They do not have data that tells them what that number is.)
- Encourage careful monitoring of all people being treated for depression.
- Extend language in the black box to indicate that the increased risk of suicidal thoughts or behaviors extends to around age 25, where it starts to drop off and become a decreased risk in the 30's and up.
- Encourage collection of data on the "activation syndrome" that some people get when taking antidepressant medications, especially SSRI's.
- Encourage collection of data which differentiates between suicidal thoughts and suicidal behaviors.
More later this evening.
6 comments:
It doesn't seem like they really stratified patients on severity of depression (I have to say, I didn't read the whole thing, I lost the will to finish it part-way in). I'm not sure how to rate severity of depression (but there must be a way other than good, bad, and ugly).
Also, with respect to the statistics, if they had used a 1-tailed hypothesis, it would have made more of their results significant. Admittedly, the 2-tailed hypothesis is the more conservative way to go, and probably more appropriate, but I was thinking about it. I was tempted to go back through and recalculate the statistics, but then I recovered my sanity.
However, one cannot differentiate between the people that have decreased suicidal ideation from antidepressant use alone, or merely from the maturity and perspective that comes from getting older.
My former shrink said I would probaby "outgrow" the borderline personality disorder by 40. I assume I would "outgrow" the chronic suicidality that comes with that DX as well.
We'll see.
This is all interesting information, but a bit intimidating for your non-shrink readers, it's not that we aren't interested.
Lily
PS Dr. McShrinky asked me if I "missed" being suicidal last time I saw him. The lithium at first got rid of the thoughts completely, but even though they are back, the urgency/intensity isn't.
ShrinkRap Readers:
How's about you nominate ShrinkRap for a Medical Blog Award?
Go here now :
http://www.medgadget.com/archives/2006/12/the_2006_medical_blog_awards.html
Welcome to the third annual Medical Weblog Awards! These awards are designed to honor the very best in the medical blogosphere, and to highlight the diverse world of medical blogs.
The categories for this year's awards will be:
-- Best Medical Weblog
-- Best New Medical Weblog (established in 2006)
-- Best Literary Medical Weblog
-- Best Clinical Sciences Weblog
-- Best Health Policies/Ethics Weblog
-- Best Medical Technologies/Informatics Weblog
-- Best Patient's Blog (a new category this year)
Nominations are now accepted in the comment section of this post. When nominating, please indicate blog's name and URL. A blog can participate in more than one category, so please indicate which one(s).
The following timeline will be observed:
-- Nominations will be accepted until Sunday, December 31, 2006.
-- Polls will be open from Wednesday, January 3, 2007 and will close at midnight on Sunday, January 14, 2007 (PST).
-- Awards will be announced on Friday, January 19, 2007.
Call me skeptical, but I am concerned that the FDA accepted data for this analysis from the drug manufacturers without checking it. Healy has shown drug company suicide data in the past to be distorted, as suicides/suicide attempts on placebo washout were inappropriately assigned to placebo. You can read my post for more details. It's possible that the data FDA analyzed were accurate, but I think there were, at the least, some coding procedures that favored medication over placebo in terms of safety.
Any who has studied this topic in depth can tell you that anti-depressant drugs can actually create suicidal thoughts and BEHAVIOR!!! Thoughts that never existed before the patient took the antidepressants drug. Hello, lets be realistic, and stop being brainwashed by the money hungery drug companies and the FDA. These two establishments has been working side by side for years, they play golf together and talk about how they can sell more drugs to increase profits. They are not interested in a cure to depression, they want to sell drugs and make money. FDA scientific research discovered the danagers of these drugs in the early 90's, but the finding were only hidden by the FDA to protect profits. Yes the government too profits tremendously off pharmasuticals. My sister was a genuine happy person her entire life. After graduating college she became restless and was experiencing early signs of depression. Her doctor prescribed her to paxil. After taking the drug for a week my sister took her own life at age 23. My sister would still be alive today if she had never taken this antidepressant. And this is not a isolated inncodent, it is very widespread. To all readers I suggest you do further research on this topic. And face the reality that the FDA and there good friend at Glaxosmithklien and the like do not care about their customers health, or lives for that matter, but they put profits first. Yes greed is an evil thing.
Anyone who wishes to comment on this blog can contact me by e-mail:
winmastaflex@aol.com
p.s., My family has attened numerous FDA hearings
Post a Comment